The San Francisco Indicators Project and Community Indicators Victoria are well-known tools that provide great lessons.
The indicator tools set up by public health teams in San Francisco (USA) and Victoria (Australia) have been widely used for built environment purposes. These projects provide useful lessons for organisations that are considering developing a new set of indicators.
Key findings about indicator use in these case studies (1):
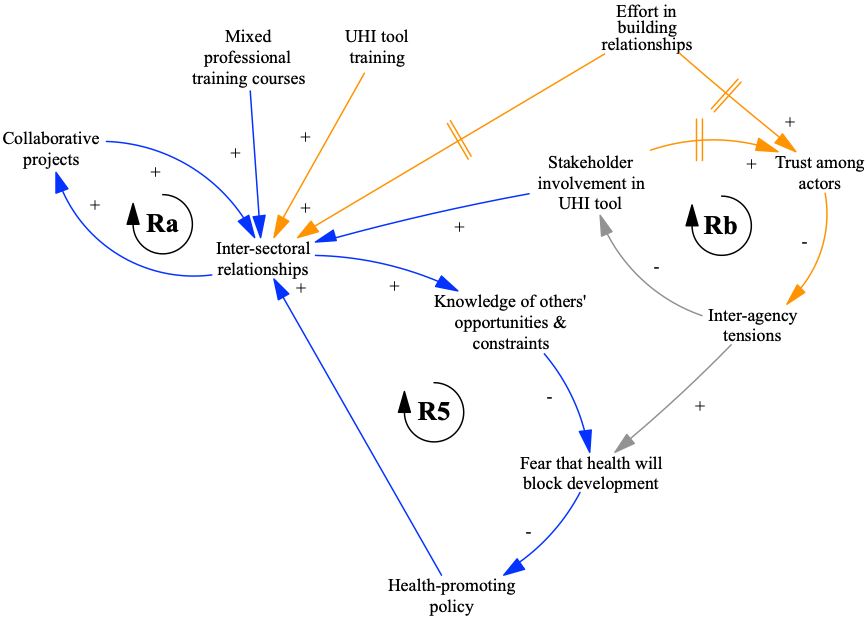
Inter-sectoral relationships were important: In the cases analysed, creating and using urban health indicator tools increased inter-sectoral relationships, which supported actors to better understand each other’s opportunities and constraints. These relationships spurred new advocates for health in diverse organisations, supporting health-in-all-policies and whole-of-society approaches.
Community involvement helped overcome constraints: When using urban health indicator tools to advocate for a healthier environment, there can be challenges. In these case studies constraints to health-promoting policy and implementation included those which were legal, political and economic in nature. Community involvement developing and using the indicators helped to overcome these constraints and supported advocacy.
Pitfalls of indicator projects: A number of factors reduced the perceived relevance and authority of indicator tools, including: a high number of available indicators, lack of neighbourhood scale data and poor-quality data.
These indicator tools were used as a form of evidence that influenced local urban planning policy and decision-making when they were embedded in policy processes, networks and institutions.
Do other indicators get used in practice?
Beyond the two examples above, does the time and effort put into developing indicators, pay off?
Looking across the published literature, here are the key findings about the use of indicators by built environment policy-makers (2).
Who creates the tools matters: Both expert-led and participatory indicator projects can be underpinned by research evidence and residents’ knowledge. Participatory UHI tools with community involvement were generally more effective at supporting “health in all policies” and “whole-of-society” approaches to governing healthy cities than expert-led processes.
Indicator use in policy-making is not linear: Studies highlighted a number of technical, organisational, political, knowledge, and contextual factors that affect their use.
Quality matters: Some indicator tool features, such as availability of neighbourhood-scale data, were influential in the use of indicators by built environment policy- and decision-makers.
References
(1) Pineo, H., Zimmermann, N., Davies, M., 2020. Integrating health into the complex urban planning policy and decision-making context: a systems thinking analysis. Palgrave Communications 6, 1–14. https://doi.org/10.1057/s41599-020-0398-3
(2) Pineo, H., Glonti, K., Rutter, H., Zimmermann, N., Wilkinson, P. and Davies, M. (2018b) Urban Health Indicator Tools of the Physical Environment: a Systematic Review. Journal of Urban Health. 95 (5), pp. 613–646. https://doi.org/10.1007/s11524-018-0228-8
Further information
Bhatia, R., 2014. Case Study: San Francisco’s Use Of Neighborhood Indicators To Encourage Healthy Urban Development. Health Affairs 33, 1914–22. http://dx.doi.org.libproxy.ucl.ac.uk/10.1377/hlthaff.2014.0661
Davern, M.T., Gunn, L., Giles-Corti, B., David, S., 2017. Best Practice Principles for Community Indicator Systems and a Case Study Analysis: How Community Indicators Victoria is Creating Impact and Bridging Policy, Practice and Research. Soc Indic Res 131, 567–586. https://doi.org/10.1007/s11205-016-1259-8
Farhang, L., Bhatia, R., Scully, C.C., Corburn, J., Gaydos, M., Malekafzali, S., 2008. Creating Tools for Healthy Development: Case Study of San Franciscoʼs Eastern Neighborhoods Community Health Impact Assessment. Journal of Public Health Management and Practice 14, 255–265. https://doi.org/10.1097/01.PHH.0000316484.72759.7b